Histopathological Spectrum of Primary Non-Small Cell Lung Carcinomas and Metastatic Carcinomas to Lung in Bronchoscopic Biopsies: Immunohistochemical and Molecular Profiling Study
- Akhtar Un Nisa Salaria , Assistant Professor, Department of Pathology, Govt. Medical College Jammu
- Bharti Devi Thaker , Associate Professor, Department of Pathology, Govt. Medical College Jammu
- Anu Radha , Assistant Professor, Department of Radiodiagnosis, Rama Medical College Hospital & Research Centre, Hapur. (Corresponding Author)
- Subash Bhardwaj , Professor. & Ex. Head Department of Pathology, Govt. Medical College Jammu
Article Information:
Abstract:
Background: Lung cancer is the leading cause of cancer-related mortality worldwide, with non-small cell lung carcinoma (NSCLC) accounting for nearly 85% of cases. The increasing reliance on bronchoscopic biopsies necessitates accurate histological subtyping and molecular characterisation on limited tissue samples, as emphasised in the World Health Organisation (WHO) 2021 classification. Materials: A retrospective observational study was conducted on 210 bronchoscopic lung biopsy specimens diagnosed as primary NSCLC or metastatic carcinomas to the lung. Initial diagnosis was based on hematoxylin and eosin (H&E) morphology. Immunohistochemistry (IHC) was applied selectively in poorly differentiated tumors, NSCLC-not otherwise specified (NOS) cases, and suspected metastases. Molecular profiling was performed in lung adenocarcinoma cases to detect actionable driver mutations. Results: Squamous cell carcinoma was the most frequent provisional diagnosis (106 cases), followed by adenocarcinoma (44 cases) and NSCLC-NOS (30 cases). IHC enabled definitive reclassification of 86.7% of NSCLC-NOS cases and all poorly differentiated carcinomas. Final diagnosis showed squamous cell carcinoma in 124 cases (59%) and adenocarcinoma in 72 cases (34.3%). Driver mutations were detected in 24 adenocarcinoma cases, with EGFR mutations being the most common (41.7%), followed by KRAS (29.2%), ALK (16.7%), BRAF (8.3%), and MET exon 14 alterations (4.1%). Conclusion: A morphology-first diagnostic strategy supplemented by judicious immunohistochemistry and molecular profiling allows accurate classification of lung tumors on bronchoscopic biopsies, optimal tissue utilisation, and facilitates personalised therapy.
Keywords:
Article :
Introduction:
Lung cancer remains the most common cause of cancer-related deaths globally and represents a major public health challenge [1,2]. Non-small cell lung carcinoma (NSCLC) comprises approximately 85% of lung cancers and includes histologically and molecularly distinct subtypes, predominantly adenocarcinoma and squamous cell carcinoma, with differing therapeutic implications [3].
With the advent of targeted therapy and immunotherapy, accurate histological subtyping and molecular characterization have become mandatory for optimal patient management [4,5]. The WHO 2021 classification of thoracic tumors underscores a morphology-first diagnostic approach, followed by selective use of immunohistochemistry (IHC) and molecular testing, particularly in small biopsy specimens [1,6].
Bronchoscopic biopsies often yield limited tissue, increasing diagnostic uncertainty and resulting in categories such as NSCLC-NOS or poorly differentiated carcinoma when morphology alone is used [7,8]. Immunohistochemical markers such as TTF-1, Napsin-A, p40, and CK5/6 have been validated as reliable tools for distinguishing adenocarcinoma from squamous cell carcinoma in small biopsies [9–11]. Additionally, molecular testing for actionable driver mutations—including EGFR, ALK, KRAS, BRAF, and MET exon 14 alterations—is now standard of care in lung adenocarcinoma, especially in Asian and Indian populations where EGFR mutation prevalence is high [12–15].
This study analyses the histopathological spectrum of primary NSCLC and metastatic carcinomas to the lung diagnosed on bronchoscopic biopsies, evaluates the diagnostic contribution of immunohistochemistry, and assesses the molecular profile of lung adenocarcinomas.
Materials and Methods:
Study Design & Causes
A retrospective observational study was conducted on 210 bronchoscopic lung biopsy specimens.
Inclusion & Exclusion criteria:
Only treatment-naïve patients with histologically confirmed NSCLC or metastatic carcinomas to the lung were included. Cases with inconclusive biopsy reports, recurrent tumors, or prior treatment were excluded.
Clinical Data
Clinical parameters included age, sex, and smoking status. Never-smokers were defined as individuals who had smoked fewer than 100 cigarettes in their lifetime.
Histopathological Evaluation
All biopsy specimens were formalin-fixed and paraffin-embedded. Initial diagnosis was rendered on H&E-stained sections.
Immunohistochemistry
IHC was applied in NSCLC-NOS cases, poorly differentiated carcinomas, and tumors suspected to be metastatic, using lineage-specific and organ-specific markers as appropriate [9,10].
Molecular Profiling
Molecular testing was performed in lung adenocarcinoma cases using RT-PCR and IHC. Driver mutations evaluated included EGFR, KRAS, ALK, BRAF, and MET exon 14 alterations, following CAP–IASLC–AMP recommendations [16,17].
Results:
Clinicodemographic Profile
The study included 210 patients, of whom 168 (80%) were males and 42 (20%) were females. The median age was 62 years (range: 21–89 years). Ninety patients (42.9%) had a history of smoking (Table 1).
Table 1. Clinicodemographic Characteristics of the Study Population (n = 210)
|
Variable |
Number (%) |
|
Total cases |
210 |
|
Male |
168 (80.0) |
|
Female |
42 (20.0) |
|
Median age (years) |
62 (range: 21–89) |
|
Smokers |
90 (42.9) |
|
Non-smokers |
120 (57.1) |
Histopathological Diagnosis and IHC Correlation
Initial H&E diagnosis showed squamous cell carcinoma in 106 cases, adenocarcinoma in 44 cases, NSCLC-NOS in 30 cases, poorly differentiated carcinoma in 20 cases, adenosquamous carcinoma in 2 cases, and metastatic tumors in 3 cases (Table 2).
Table 2. Initial Histopathological Diagnosis on H&E and Immunohistochemical (IHC) Correlation
|
Initial H&E Diagnosis |
No. of Cases |
IHC-Based Final Diagnosis |
|
Squamous cell carcinoma |
106 |
All confirmed as well/moderately differentiated squamous cell carcinoma |
|
Adenocarcinoma |
44 |
All confirmed as well/moderately differentiated adenocarcinoma |
|
NSCLC-NOS / Undifferentiated carcinoma |
30 |
20 adenocarcinoma |
|
Poorly differentiated carcinoma |
20 |
12 squamous cell carcinoma |
|
Adenosquamous carcinoma |
2 |
Both confirmed as adenosquamous carcinoma |
|
Metastatic tumors to lung |
3 |
1 gastrointestinal adenocarcinoma |
Immunohistochemistry enabled significant diagnostic refinement. Among 30 NSCLC-NOS cases, 20 were reclassified as adenocarcinoma, 6 as squamous cell carcinoma, and 4 retained a null phenotype. All poorly differentiated carcinomas were lineage-assigned (12 squamous cell carcinoma, 8 adenocarcinoma). Metastatic tumors were accurately characterized using organ-specific markers.
The final histological classification after IHC integration is shown in Table 3. Squamous cell carcinoma constituted 59% of cases, while adenocarcinoma accounted for 34.3%. The diagnostic utility of IHC in ambiguous tumors is summarized in Table 4.
Table 3. Final Histological Classification After IHC Integration
|
Final Diagnosis |
Number of Cases (%) |
|
Squamous cell carcinoma |
124 (59.0) |
|
Adenocarcinoma |
72 (34.3) |
|
Adenosquamous carcinoma |
2 (1.0) |
|
Null phenotype carcinoma |
4 (1.9) |
|
Metastatic tumors to lung |
3 (1.4) |
|
Total |
210 (100) |
Table 4. Diagnostic Utility of Immunohistochemistry in Ambiguous Tumors
|
Diagnostic Category |
Number of Cases |
Correctly Classified on IHC (%) |
|
NSCLC-NOS |
30 |
26 (86.7) |
|
Poorly differentiated carcinoma |
20 |
20 (100) |
Histological Patterns of Adenocarcinoma
Among 72 adenocarcinoma cases, acinar (37%) and solid (27%) patterns were most frequent, followed by micropapillary, papillary, lepidic, and enteric patterns (Table 5).
Table 5. Histological Patterns of Lung Adenocarcinoma (n = 72)
|
Histological Pattern |
Number of Cases (%) |
|
Acinar |
26 (37.0) |
|
Solid |
20 (27.0) |
|
Micropapillary |
10 (14.0) |
|
Papillary |
7 (10.0) |
|
Lepidic |
6 (8.0) |
|
Enteric type |
3 (4.0) |
Molecular Profiling
Driver mutations were detected in 24 adenocarcinoma cases. EGFR mutations were most common (41.7%), followed by KRAS (29.2%), ALK (16.7%), BRAF (8.3%), and MET exon 14 alterations (4.1%). Molecular alterations are detailed in Table 6.
Table 6. Molecular Alterations Detected in Lung Adenocarcinoma (n = 24)
|
Driver Mutation |
Number of Patients |
Percentage (%) |
|
EGFR |
10 |
41.7 |
|
KRAS |
7 |
29.2 |
|
ALK |
4 |
16.7 |
|
BRAF |
2 |
8.3 |
|
MET exon 14 |
1 |
4.1 |
Discussion:
Accurate classification of lung cancer on bronchoscopic biopsy specimens remains challenging due to limited tissue and tumor heterogeneity. In the present study, nearly one-fourth of cases were initially categorised as NSCLC-NOS or poorly differentiated carcinoma on morphology alone, consistent with previous reports [7,8].
The application of a focused immunohistochemical panel enabled definitive lineage assignment in 86.7% of NSCLC-NOS cases and all poorly differentiated carcinomas (Table 4). This finding aligns with earlier studies demonstrating the effectiveness of selective IHC in small biopsy specimens while preserving tissue for molecular testing [7,18].
Squamous cell carcinoma was the predominant subtype in our cohort (Table 3), reflecting smoking-associated lung cancer patterns reported in Indian studies [14,19]. Morphological features of well-differentiated squamous cell carcinoma were evident on H&E sections (Figure 1), while poorly differentiated variants required immunohistochemical confirmation (Figure 2).
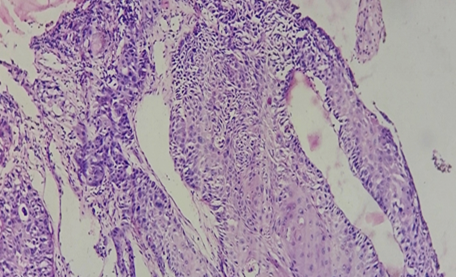
Figure 1: Well-differentiated squamous cell carcinoma of lung showing nests of malignant squamous cells with keratin pearl formation (H&E 40X).
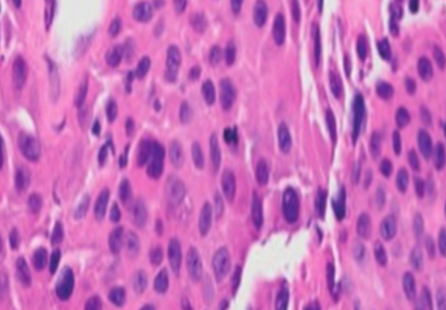

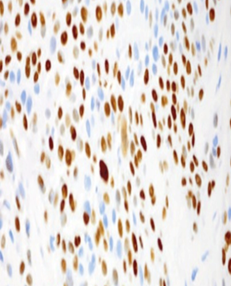
Figure 2: Poorly differentiated squamous cell carcinoma with sheets of pleomorphic tumor cells (A) H&E 40X), showing CK 5/6 Cytoplasmic positivity (B) and nuclear p40 positivity (C).
Adenocarcinoma constituted approximately one-third of cases, with acinar and solid patterns being most frequent (Table 5). Micropapillary and lepidic patterns, which carry prognostic significance, were identifiable even in small biopsy samples (Figures 3 and 4), highlighting the diagnostic adequacy of bronchoscopic biopsies when optimally processed.
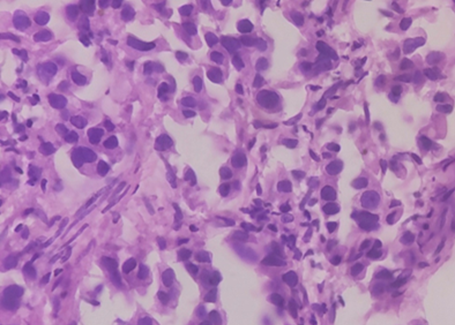
Figure 3: Micropapillary adenocarcinoma of lung showing small clusters of tumor cells lacking fibrovascular cores (H&E 40X).
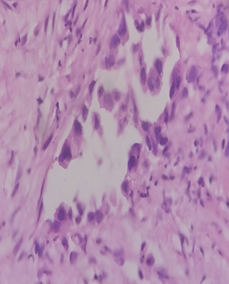
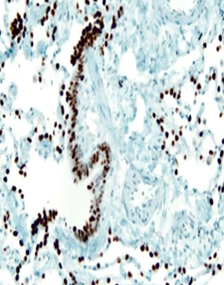
Figure 4: Adenocarcinoma Lung lepidic type(A) H&E 40X and TTF 1 positivity(B).
Metastatic tumors to lung, though infrequent, were accurately identified using organ-specific immunomarkers (Figures 5–7). This emphasizes the importance of clinical correlation and targeted IHC to avoid misclassification of metastases as primary lung tumors [20,21].
Molecular profiling revealed actionable driver mutations in one-third of adenocarcinoma cases (Table 6). The high frequency of EGFR mutations (41.7%) is consistent with Indian and Asian studies, underscoring the importance of routine EGFR testing in lung adenocarcinoma [12–15]. Detection of KRAS, ALK, BRAF, and MET exon 14 alterations further highlights the molecular heterogeneity of lung adenocarcinoma and the therapeutic relevance of comprehensive molecular testing [22–25].
Overall, our findings support the WHO 2021 and CAP–IASLC–AMP guidelines advocating an integrated diagnostic approach combining morphology, immunohistochemistry, and molecular profiling in small biopsy specimens [1,16,17].
Limitations
The retrospective design and lack of survival or treatment outcome data are acknowledged limitations. Expanded next-generation sequencing and uniform PD-L1 testing were not available in all cases, reflecting real-world constraints in resource-limited settings [17,26].
Conclusion:
Immunohistochemistry is indispensable for refining lung cancer diagnosis on bronchoscopic biopsies, particularly in NSCLC-NOS and poorly differentiated tumors. Molecular profiling of lung adenocarcinomas reveals actionable driver mutations in a substantial proportion of cases. A morphology-first, tissue-sparing diagnostic algorithm ensures accurate classification and facilitates personalized therapy.
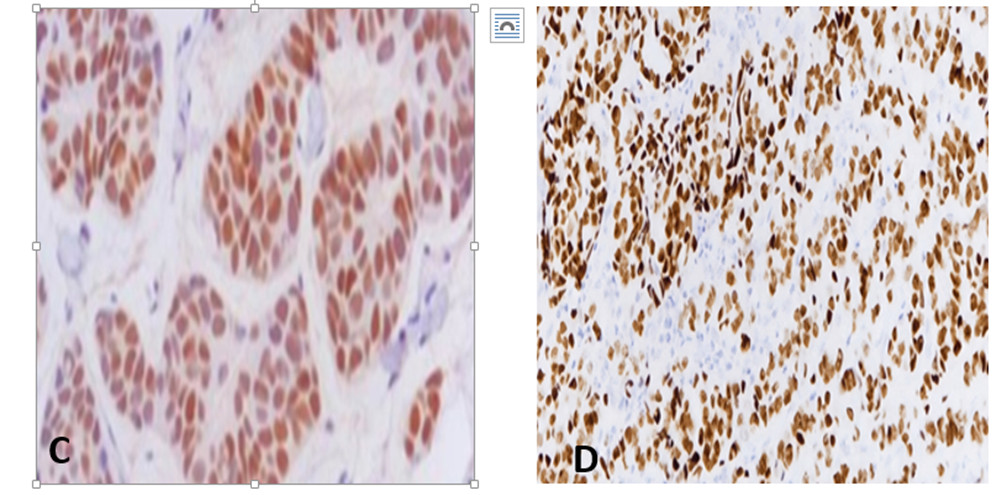
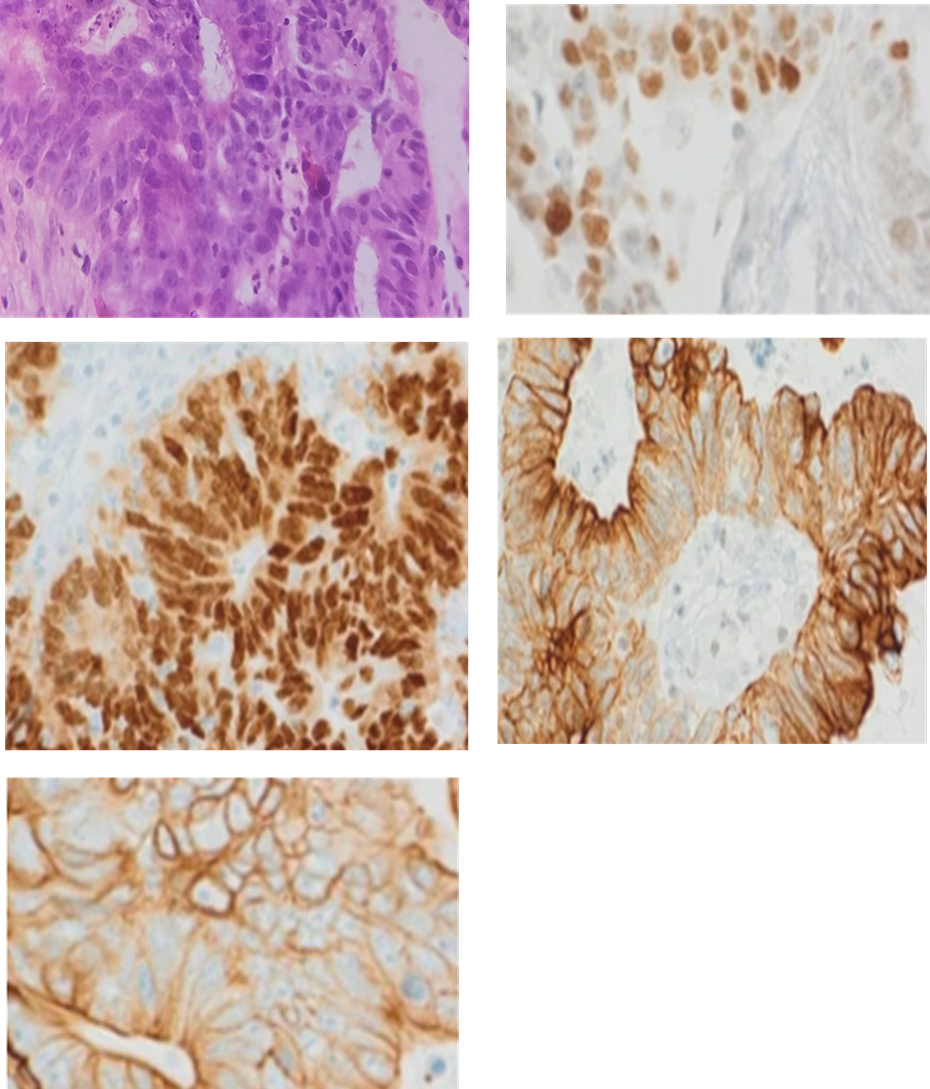
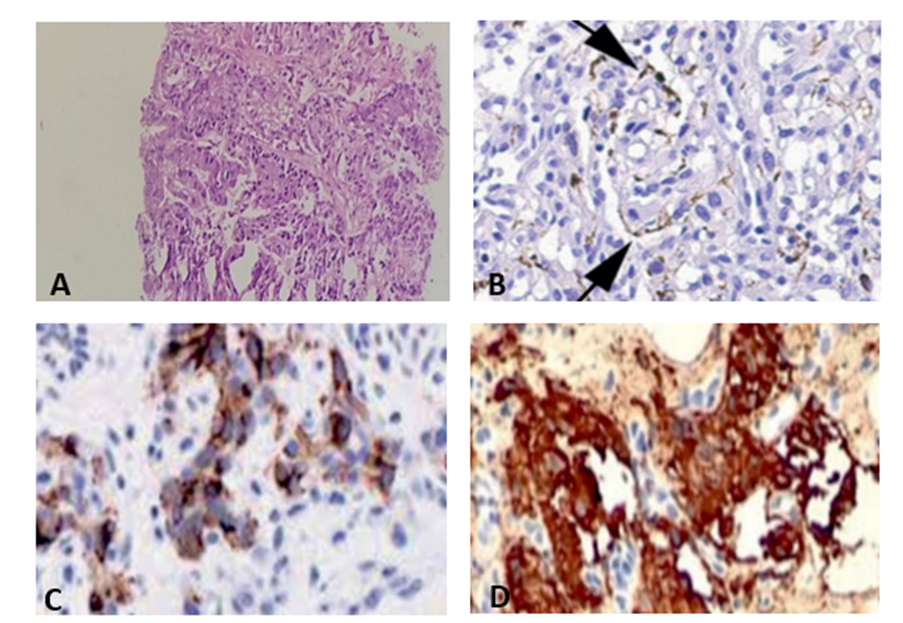
Figure 7: Metastatic paraganglioma involving lung showing (A) Zell Ballen pattern (H&E, 40X) with sustentacular cells highlighted by S-100 (B), Chromogranin positivity (C) and synaptophysin positivity (D).
References:
1. Nicholson AG, Tsao MS, Beasley MB, Borczuk AC, Brambilla E, Cooper WA, et al. The 2021 WHO classification of lung tumors: impact of advances since 2015. J Thorac Oncol. 2022;17(3):362-387.
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
3. Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG. Introduction to the 2015 World Health Organization classification of tumors of the lung, pleura, thymus, and heart. Arch Pathol Lab Med. 2015;139(5):589-600.
4. Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ Jr, Wu YL, et al. Lung cancer: current therapies and new targeted treatments. Lancet. 2017;389(10066):299-311.
5. Scagliotti GV, Parikh P, von Pawel J, Biesma B, Vansteenkiste J, Manegold C, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naïve patients with advanced-stage non–small-cell lung cancer. Lancet Oncol. 2008;9(1):43-54.
6. Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6(2):244-285.
7. Travis WD, Rekhtman N, Riley GJ, Geisinger KR, Asamura H, Brambilla E. Pathologic diagnosis of lung cancer in small biopsies and cytology: challenges, limitations, and recommendations. Arch Pathol Lab Med. 2013;137(5):668-684.
8. Rossi G, Marchioni A, Romagnani E, Bertolini F, Longo L, Cavazza A, et al. Primary lung cancer: small biopsies and cytology—diagnosis, molecular testing and personalized therapy. Virchows Arch. 2014;464(2):133-148.
9. Rekhtman N. Immunohistochemistry in lung cancer: what, why, and when. Arch Pathol Lab Med. 2010;134(12):1758-1764.
10. Yatabe Y, Dacic S, Borczuk AC, Warth A, Russell PA, Lantuejoul S, et al. Best practices recommendations for diagnostic immunohistochemistry in lung cancer. J Thorac Oncol. 2019;14(3):377-407.
11. Bishop JA, Teruya-Feldstein J, Westra WH. p40 (ΔNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Am J Surg Pathol. 2012;36(9):1392-1399.
12. Chougule A, Prabhash K, Noronha V, Joshi A, Jambhekar N. Frequency of EGFR mutations in Indian patients with non–small-cell lung cancer. J Thorac Oncol. 2013;8(4):S336-S337.
13. Doval DC, Prabhash K, Patil S, Batra U, Chaturvedi H, Goswami C, et al. Molecular profiling of advanced non–small-cell lung cancer in Indian patients. Indian J Cancer. 2019;56(2):152-159.
14. Arora A, Kumar A, Gupta N, Khilnani GC. Clinicopathological profile of lung cancer in north India. Lung India. 2016;33(6):598-603.
15. Noronha V, Patil VM, Joshi A, Menon N, Chougule A, Prabhash K. Lung cancer in India: current status and promising strategies. South Asian J Cancer. 2016;5(3):93-98.
16. Lindeman NI, Cagle PT, Aisner DL, Arcila ME, Beasley MB, Bernicker EH, et al. Updated molecular testing guideline for the selection of lung cancer patients for treatment with targeted tyrosine kinase inhibitors. J Thorac Oncol. 2018;13(3):323-358.
17. Lindeman NI. Tissue stewardship in lung cancer diagnosis and molecular testing. Arch Pathol Lab Med. 2019;143(2):122-127.
18. Rekhtman N. Lung carcinoma classification issues in small biopsies and cytology specimens. Semin Diagn Pathol. 2015;32(6):518-535.
19. Behera D, Balamugesh T. Lung cancer in India. Indian J Chest Dis Allied Sci. 2004;46(4):269-281.
20. Ordóñez NG. Value of immunohistochemistry in distinguishing primary tumors from metastatic tumors in the lung. Adv Anat Pathol. 2012;19(1):3-24.
21. Suster S. Metastatic tumors of the lung. Semin Diagn Pathol. 1995;12(2):126-138.
22. Paik PK, Arcila ME, Fara M, Sima CS, Miller VA, Kris MG, et al. Clinical characteristics of patients with lung adenocarcinomas harboring KRAS mutations. Clin Cancer Res. 2011;17(17):5543-5550.
23. Gainor JF, Varghese AM, Ou SHI, Kabraji S, Awad MM, Katayama R, et al. ALK rearrangements are mutually exclusive with mutations in EGFR or KRAS in lung adenocarcinoma. Cancer Discov. 2013;3(3):287-299.
24. Planchard D, Smit EF, Groen HJM, Mazieres J, Besse B, Helland Å, et al. Dabrafenib plus trametinib in patients with BRAF V600E-mutant metastatic non–small-cell lung cancer. Ann Oncol. 2017;28(2):362-368.
25. Awad MM, Oxnard GR, Jackman DM, Savukoski DO, Hall D, Shivdasani P, et al. MET exon 14 mutations in non–small-cell lung cancer are associated with advanced age and distinct genomic profiles. Cancer Discov. 2016;6(12):1334-1342.