Effectiveness of a Cartoon Animation-Based Oral Health Education Tutorial in Promoting Oral Health Status Among 6- to 9-Year-Old School-Going Children in Chennai City: An Interventional Study.
- Bijivin Raj Vethakkan , Associate Professor, Department of Dentistry, Kanyakumari Medical Mission Research Centre, Muttom, Kanyakumari, Tamil Nadu, India.
- Sivalingam S , Assistant Professor, Department of Community Medicine, Kanyakumari Medical Mission Research Centre, Muttom, Kanyakumari, Tamil Nadu, India.
- Junaid Naina M , Associate Professor , Department of Pharmacology, Azeezia Institute of Medical Sciences and Research, Kollam,Kerala, India.
- Guganandaprabu Velu , Dentist and Medical Professional Legal Consultant, Head of Medical Records Department and Transcription, The Guardian Group LLC, California, USA.
Article Information:
Abstract:
Background: Dental plaque is a modifiable risk factor for both dental caries and gingival inflammation, and school-based oral health education remains a practical strategy for establishing healthy behaviours early in life. Interactive digital media could strengthen message retention among younger children. Objectives: To assess the effectiveness of a cartoon animation-based oral health education tutorial in improving oral hygiene status among 6- to 9-year-old school-going children and to compare its effect with that of traditional oral health education. Methods: This parallel-arm interventional study was conducted among 100 children aged 6-9 years in Chennai city. Children were randomly allocated into two equal groups. Group A received a traditional oral health education lecture, whereas Group B received the same lecture plus a 2-minute cartoon animation-based toothbrushing tutorial reinforced daily for 6 weeks. Plaque Index and Gingival Index were recorded at baseline, at 6 weeks, and at 12 weeks. Non-parametric tests were used for repeated assessments across time points. Results: The mean age of the participants was 7.7±0.915 years. Both groups showed improvement after intervention, but the reduction was markedly greater in the animation group. Plaque scores in Group A changed from 1.30 at baseline to 1.24 post-intervention and 1.27 at follow-up, whereas Group B improved from 1.20 to 0.57 and 0.65, respectively. Gingival scores in Group A changed from 1.19 to 1.10 and 1.18, while Group B improved from 1.34 to 0.91 and 1.05. Within-group changes were statistically significant, with stronger and more sustained improvement in the animation group. Conclusion: Cartoon animation-based oral health education produced better short-term and follow-up oral hygiene outcomes than traditional lecture-based education alone. Reinforced, child-friendly visual instruction appears to be an effective strategy for improving plaque control and gingival health in younger school children.
Keywords:
Article :
INTRODUCTION:
Oral health is an essential component of general health, functional well-being, and quality of life.[1] Oral diseases continue to impose a substantial public health burden worldwide, particularly among children, because of their high prevalence, recurrent nature, and impact on eating, speaking, appearance, social interaction, and school participation.[2] Dental plaque plays a central role in the initiation of both dental caries and gingival inflammation. Establishing effective plaque-control practices during childhood is therefore a critical preventive priority. Evidence shows that early and regular oral hygiene habits, especially toothbrushing with fluoride toothpaste, are associated with better oral health outcomes.[3] Supervised toothbrushing and structured oral health education have also been shown to improve oral hygiene status among school-aged children.[4]
School settings offer a valuable platform for health promotion because children can be reached repeatedly during a formative period of behavioural development.[2,4] Toothbrushing, although simple in principle, requires correct technique, repetition, motivation, and reinforcement. Habit studies indicate that while many children report brushing at least once or twice daily, the consistency and quality of brushing remain variable, leaving scope for educational reinforcement.[5] Conventional oral health education, typically delivered through lectures or verbal instruction, can improve knowledge; however, its influence on sustained behavioural change is often modest unless the messages are repeated and made developmentally engaging.[6-8] This gap is especially important in younger children, who respond more readily to imitation, play, rhythm, repetition, and visually guided routines than to abstract verbal advice alone.
Visual learning tools have increasingly been used to support health education among children. Animated and interactive media can simplify complex messages, capture attention, improve recall, and convert routine health instructions into appealing behavioural cues. Prior studies have shown that school-based interventions using printed or audiovisual educational tools can reduce plaque accumulation and improve gingival health.[7-11] Similarly, visually adapted oral health education has been effective in children with communication challenges, highlighting the value of engaging and understandable educational formats.[12] Even so, evidence remains limited regarding interactive cartoon animation tutorials designed specifically for younger schoolchildren and reinforced in the home environment.
Against this background, the present study was undertaken to evaluate whether a cartoon animation-based oral health education tutorial could produce greater improvement in oral hygiene status than traditional oral health education among 6- to 9-year-old school-going children in Chennai city. The specific objectives were to assess changes in Plaque Index and Gingival Index following the intervention and to compare these changes between children exposed to traditional oral health education alone and those receiving additional cartoon animation-based reinforcement.
MATERIALS AND METHODS:
Study design and setting. A parallel-arm interventional study was carried out among school-going children aged 6-9 years in Chennai city. Ethical clearance was obtained from the institutional review board before the start of the study. The study protocol was also registered in the Clinical Trial Registry of India (CTRI/REF/2017/11/015971). Written bilingual informed consent was obtained from parents or guardians after they had read the participant information sheet
.Participants and sampling. The source population comprised children studying in the 2nd, 3rd, and 4th standards. A list of 184 children was prepared, and simple random sampling was used to recruit participants who satisfied the eligibility criteria. The final sample consisted of 100 children, with 50 allocated to each study arm. Children were eligible if their parents consented to participation, if the child had a normal intellectual profile, was able to understand and follow toothbrushing instructions, brushed independently, and belonged to a household using a smartphone or tablet. Children with chronic dental or systemic disease, those receiving medication, and those who had undergone dental treatment within the previous three months were excluded.
Intervention procedures. A single calibrated investigator delivered both interventions and completed the recording proforma. A pilot study was conducted two weeks before the main study. Baseline demographic details were recorded through the respective class teachers on the day of examination. All children underwent intra-oral examination at baseline. Group A received a traditional oral health education lecture delivered in Tamil using simple, non-technical language. The session lasted approximately 30 minutes and covered the importance of oral hygiene, frequency of brushing, and correct brushing practice. Group B received the same lecture in addition to a cartoon animation-based toothbrushing tutorial.
Cartoon animation tutorial. The animation was a two-dimensional 2-minute video featuring an interactive monkey character that demonstrated the recommended circular toothbrushing technique. The tutorial incorporated child-friendly visuals and a brushing rhyme to increase attention and enjoyment. Parents were instructed to display the video daily for 7 days each week for 6 weeks. After completion of the intervention phase, parents were asked not to show the video during the subsequent 6-week follow-up period, allowing post-reinforcement behaviour to be assessed.
Outcome assessment and statistical analysis. Oral health status was evaluated at baseline, at the end of the 6-week intervention, and again after the 6-week follow-up period. Plaque Index was recorded using the Silness and Loe index,[13] and gingival status was assessed using the Loe and Silness Gingival Index.[14] Data were entered and analysed using Statistical Package for the Social Sciences (SPSS) version 20.0. Descriptive statistics were expressed as mean and standard deviation. Because the variables did not follow a normal distribution, non-parametric methods were used. Between-group comparisons were performed using the Mann-Whitney U test, and repeated within-group comparisons across baseline, post-intervention, and follow-up assessments were evaluated using Friedman and Wilcoxon signed-rank procedures. A p value of less than 0.05 was considered statistically significant.
RESULTS:
A total of 100 children were included in the analysis, with 50 participants in each group. The overall mean age of the study population was 7.7 ± 0.9 years. Group A comprised 22 boys and 28 girls, whereas Group B included 24 boys and 26 girls, indicating a broadly similar sex distribution between the two study arms [Table 1].
Table 1. Baseline characteristics of the study population
|
Variable |
Category |
Group A (n = 50) |
Group B (n = 50) |
|
Age, years |
Mean ± SD |
Overall sample: 7.7 ± 0.9 |
Overall sample: 7.7 ± 0.9 |
|
Sex |
Boys/Girls |
22/28 |
24/26 |
Values are presented as mean ± SD or number of participants.
Plaque Index scores decreased after the intervention in both groups; however, the magnitude of improvement was considerably greater in the children who received the cartoon animation tutorial. In Group A, the mean Plaque Index declined slightly from 1.30 ± 0.4 at baseline to 1.24 ± 0.3 post-intervention and was 1.27 ± 0.3 at follow-up, suggesting only minimal net improvement over time. In Group B, the mean Plaque Index decreased from 1.20 ± 0.3 at baseline to 0.57 ± 0.4 post-intervention and remained low at 0.65 ± 0.5 at follow-up. The absolute reduction from baseline to post-intervention was 0.06 units in Group A compared with 0.63 units in Group B, and the corresponding reductions at follow-up were 0.03 and 0.55 units, respectively. Although a small rebound was observed during follow-up in both groups, the animation group retained most of its initial gain. The within-group change across the three assessments was statistically significant in both groups, with stronger evidence in Group B [Table 2].
Table 2. Plaque Index scores over time and absolute change from baseline
|
Group |
Baseline |
Post-intervention |
Follow-up |
Change from baseline to post |
Change from baseline to follow-up |
|
Group A |
1.30 ± 0.4 |
1.24 ± 0.3 |
1.27 ± 0.3 |
−0.06 |
−0.03 |
|
Group B |
1.20 ± 0.3 |
0.57 ± 0.4 |
0.65 ± 0.5 |
−0.63 |
−0.55 |
Within-group Friedman test p values: Group A, 0.013; Group B, <0.001. Negative values indicate reduction from baseline.
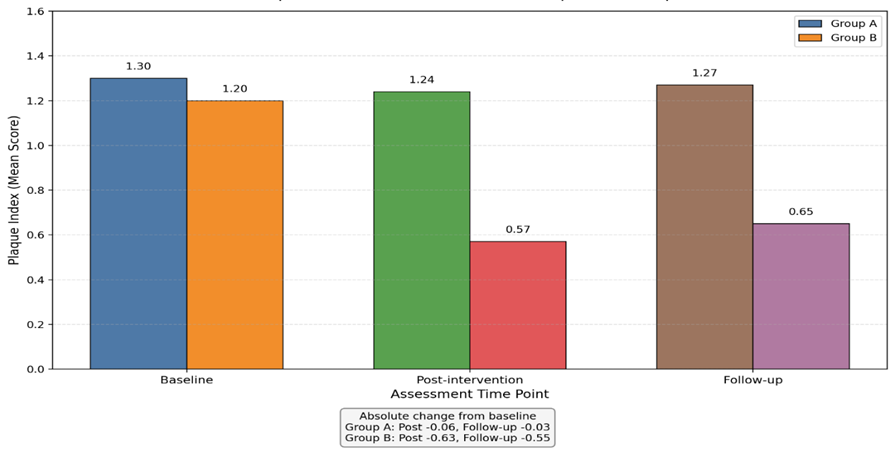
Figure 1: Plaque Index scores over time in Group A and Group B
Gingival Index scores showed a similar pattern. In Group A, the mean score decreased from 1.19 ± 0.3 at baseline to 1.10 ± 0.2 post-intervention, but increased to 1.18 ± 0.2 at follow-up, indicating that most of the initial improvement was not sustained. In Group B, the mean Gingival Index decreased from 1.34 ± 0.2 at baseline to 0.91 ± 0.2 post-intervention and was 1.05 ± 0.3 at follow-up. The absolute reduction from baseline to post-intervention was 0.09 units in Group A and 0.43 units in Group B, while the reductions from baseline to follow-up were 0.01 and 0.29 units, respectively. Thus, gingival health improved in both groups immediately after the educational intervention, but the improvement was larger and more persistent in the animation group. Friedman test results demonstrated statistically significant within-group variation over time in both groups [Table 3].
Table 3. Gingival Index scores over time and absolute change from baseline
|
Group |
Baseline |
Post-intervention |
Follow-up |
Change from baseline to post |
Change from baseline to follow-up |
|
Group A |
1.19 ± 0.3 |
1.10 ± 0.2 |
1.18 ± 0.2 |
−0.09 |
−0.01 |
|
Group B |
1.34 ± 0.2 |
0.91 ± 0.2 |
1.05 ± 0.3 |
−0.43 |
−0.29 |
Within-group Friedman test p values: Group A, <0.001; Group B, <0.001. Negative values indicate reduction from baseline.
Overall, traditional lecture-based oral health education produced only limited short-term improvement, whereas the cartoon animation tutorial was associated with substantially greater reductions in plaque accumulation and gingival inflammation. Although some attenuation of effect was observed during the non-reinforcement follow-up period, Group B continued to demonstrate better oral hygiene outcomes than Group A at the end of the study. A summary of the change scores across both indices is presented in Table 4.
Table 4. Summary of intervention-related change across oral health indices
|
Index |
Group |
Immediate reduction |
Reduction retained at follow-up |
Rebound after intervention |
Interpretation |
|
Plaque Index |
Group A |
0.06 |
0.03 |
0.03 |
Minimal improvement; most of the modest gain was lost by follow-up |
|
Plaque Index |
Group B |
0.63 |
0.55 |
0.08 |
Marked improvement with substantial retention at 12 weeks |
|
Gingival Index |
Group A |
0.09 |
0.01 |
0.08 |
Small short-term improvement with near-return to baseline |
|
Gingival Index |
Group B |
0.43 |
0.29 |
0.14 |
Greater and more sustained improvement than Group A |
DISCUSSION:
The present study showed improvement in both groups, but the change was clearly larger in the group that received the cartoon animation tutorial in addition to the conventional lecture. This pattern was evident for both plaque and gingival scores and persisted, although attenuated, after reinforcement stopped. The findings suggest that oral health education becomes more effective when it is not limited to one-time verbal instruction but is delivered in a form that children can repeatedly watch, imitate, and enjoy.[6-8]
The modest benefit observed in Group A agrees with earlier school-based studies showing that conventional dental health education improves awareness but often produces only limited behavioural change when reinforcement is infrequent.[8,9] In the present study, plaque and gingival scores in the lecture-only group improved slightly after intervention and then moved back toward baseline at follow-up. That pattern indicates that knowledge transfer alone did not sufficiently stabilize brushing performance in younger children.
The stronger improvement in Group B is consistent with reports showing better oral hygiene outcomes with reinforced audiovisual or visually adapted education. Yazdani et al. found short-term improvement in oral cleanliness and gingival health after school-based educational interventions using leaflet and videotape support.[7] Hebbal et al. also reported lower plaque scores when audiovisual aids were used than with conventional teaching.[11] Likewise, visually tailored oral health education improved clinical outcomes in children with hearing impairment, underscoring the value of educational tools that are easy to follow and imitate.[12]
Several factors probably contributed to the superior performance of the animation group. The cartoon character converted brushing instruction into an attractive behavioural cue, while the rhyme and movement likely increased attention and recall. Daily repetition at home during the six-week intervention probably strengthened motor learning of the recommended circular brushing technique. The small rebound seen at follow-up further indicates that reinforcement itself played an important role and that booster exposure would help preserve gains over time.[10]
From a practical standpoint, the intervention was brief, low-cost, and usable through devices already present in many households. It also influenced clinical outcomes rather than knowledge alone, which makes the findings more relevant for preventive dentistry. Overall, the study supports the use of child-centred digital reinforcement as a meaningful adjunct to conventional school oral health education.
Limitations
The intervention required access to smartphones or comparable digital devices and a minimum level of parental digital literacy, which restricts applicability in households without such resources. Follow-up was limited to six weeks after withdrawal of the video, so durability beyond 12 weeks remains unresolved. The source dataset provided repeated-measures significance values but not complete between-group inferential estimates, which constrained deeper comparative statistical interpretation.
CONCLUSION:
This interventional study showed that oral health education improved oral hygiene status in both study groups, but the improvement was substantially greater when traditional instruction was supplemented with a cartoon animation-based toothbrushing tutorial. Children exposed to the animated tutorial demonstrated larger reductions in plaque and gingival scores after six weeks and retained a better level of oral hygiene at follow-up despite partial rebound after reinforcement stopped. The findings indicate that visually engaging, age-appropriate, and repeatedly delivered educational media can strengthen daily toothbrushing behaviour in young schoolchildren. Incorporating such child-friendly digital tools into school oral health promotion programmes can enhance the effectiveness of preventive education and support better early oral health outcomes.
REFERENCES:
1. Baiju RM, Peter E, Varghese NO, Sivaram R. Oral health and quality of life: current concepts. J Clin Diagn Res. 2017;11(6):ZE21-ZE26.
2. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661-669.
3. Wendt LK, Hallonsten AL, Koch G, Birkhed D. Oral hygiene in relation to caries development and immigrant status in infants and toddlers. Scand J Dent Res. 1994;102(5):269-273.
4. Damle SG, Patil A, Jain S, Damle D, Chopal N. Effectiveness of supervised toothbrushing and oral health education in improving oral hygiene status and practices of urban and rural school children: a comparative study. J Int Soc Prev Community Dent. 2014;4(3):175-181.
5. Koerber A, Burns JL, Berbaum M, Punwani I, Levy SR, Cowell J, Flay B. Toothbrushing patterns over time in at-risk metropolitan African-American 5th-8th graders. J Public Health Dent. 2005;65(4):240-243.
6. Saied-Moallemi Z, Virtanen JI, Vehkalahti MM, Tehranchi A, Murtomaa H. School-based intervention to promote preadolescents' gingival health: a community trial. Community Dent Oral Epidemiol. 2009;37(6):518-526.
7. Yazdani R, Vehkalahti MM, Nouri M, Murtomaa H. School-based education to improve oral cleanliness and gingival health in adolescents in Tehran, Iran. Int J Paediatr Dent. 2009;19(4):274-281.
8. Shenoy RP, Sequeira PS. Effectiveness of a school dental education program in improving oral health knowledge and oral hygiene practices and status of 12- to 13-year-old school children. Indian J Dent Res. 2010;21(2):253-259.
9. Zimmerman M, Bornstein R, Martinsson T. Simplified preventive dentistry program for Chilean refugees: effectiveness of one versus two instructional sessions. Community Dent Oral Epidemiol. 1993;21(3):143-147.
10. Freitas-Fernandes LB, Novaes AB Jr, Feitosa AC, Novaes AB. Effectiveness of an oral hygiene program for Brazilian orphans. Braz Dent J. 2002;13(1):44-48.
11. Hebbal M, Ankola AV, Vadavi D, Patel K. Evaluation of knowledge and plaque scores in school children before and after health education. Dent Res J (Isfahan). 2011;8(4):189-196.
12. Shetty V, Kumar J, Hegde A. Breaking the sound barrier: oral health education for children with hearing impairment. Spec Care Dentist. 2014;34(3):131-137.
13. Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121-135.
14. Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533-551.