Primary Central Nervous System Lymphoma: A Retrospective Case Series of Three Patients.
- Rehana Begum , Senior Resident, Department of Neurosurgery, St. John’s Medical College and Hospital, Bengaluru.
- Rahul Jain , Senior Resident, Department of Neurosurgery, St. John’s Medical College and Hospital, Bengaluru.
- Karthik C , Senior Resident, Department of Neurosurgery, St. John’s Medical College and Hospital, Bengaluru.
- Rajesh R Raykar , Professor and Head, Department of Neurosurgery, St. John’s Medical College and Hospital, Bengaluru.
- Shailesh A V Rao , Professor, Department of Neurosurgery, St. John’s Medical College and Hospital, Bengaluru.
Article Information:
Abstract:
Background: Primary central nervous system lymphoma (PCNSL) is a rare and aggressive extranodal non-Hodgkin lymphoma confined to the brain, leptomeninges, spinal cord, or eyes without systemic disease. It represents a small proportion of CNS malignancies, and diffuse large B-cell lymphoma (DLBCL) is the predominant histological subtype.[1,2]. Materials and methods: A retrospective case series of three biopsy-proven PCNSL patients managed between November 2025 and April 2026 was conducted. Clinical presentation, radiological findings, surgical approach, histopathology, and adjuvant treatment were reviewed from institutional records. Result: The patients were aged 53 to 72 years. Headache was the most common presenting symptom. Magnetic resonance imaging demonstrated contrast-enhancing lesions with diffusion restriction in all three patients. Two patients underwent stereotactic or neuronavigation-guided biopsy, while one patient underwent subtotal resection. Histopathology confirmed DLBCL in all three cases. All patients were referred for oncological treatment. Conclusion: PCNSL should be suspected in patients with enhancing intracranial lesions showing diffusion restriction on MRI. Early tissue diagnosis by stereotactic or navigation-guided biopsy remains essential for definitive diagnosis and initiation of methotrexate-based therapy. [4,5].
Keywords:
Article :
INTRODUCTION:
Primary central nervous system lymphoma is an uncommon extranodal non-Hodgkin lymphoma arising within the brain, leptomeninges, spinal cord, or eyes in the absence of systemic lymphoma.[3,4] It accounts for approximately 1% of all lymphomas and around 1% to 4% of central nervous system malignancies.[3,4]
Most PCNSL cases are histologically classified as diffuse large B-cell lymphoma. Patients may present with headache, focal neurological deficits, cognitive impairment, neuropsychiatric symptoms, or features related to raised intracranial pressure, which often makes early diagnosis challenging.[2,3]
Magnetic resonance imaging typically shows homogeneously or heterogeneously enhancing lesions with restricted diffusion, but radiological findings may overlap with glioma, metastasis, demyelinating lesions, and infectious or inflammatory conditions.[2,3]] Therefore, histopathological confirmation remains the cornerstone of diagnosis, and surgery is generally limited to biopsy rather than extensive resection in most cases.[2,3]
The present case series describes the clinical, radiological, and histopathological profile of three patients with PCNSL treated at a tertiary care neurosurgical center and highlights the role of early tissue diagnosis in guiding treatment.
OBJECTIVES
The objective of this study was to describe the clinical presentation, imaging characteristics, operative strategy, and histopathological findings in three patients with biopsy-proven primary central nervous system lymphoma.
MATERIALS AND METHODS:
This was a retrospective case series conducted in the Department of Neurosurgery at St. John’s Medical College and Hospital. Three patients with biopsy-proven primary central nervous system lymphoma managed between November 2025 and April 2026 were included.
Inclusion criteria
· Patients aged more than 20 years.
· Histopathologically confirmed primary central nervous system lymphoma.
Exclusion criteria
· Patients younger than 20 years.
· Patients lost to follow-up.
Clinical presentation, neurological examination, magnetic resonance imaging findings, operative approach, histopathology, and subsequent oncological treatment were reviewed from hospital records. Tissue diagnosis was obtained through frame-based stereotactic biopsy, neuronavigation-guided biopsy, or craniotomy depending on lesion location and preoperative diagnostic considerations.
CASE PRESENTATION:
Case 1
A 72-year-old woman presented with headache and right-sided weakness of 10 days’ duration. She had diabetes mellitus and hypertension and was compliant with medication. On examination, Glasgow Coma Scale score was E4V5M6, pupils were equal and reactive to light, and she had right lower motor neuron facial palsy with 0/5 power in the right upper and lower limbs.
Magnetic resonance imaging revealed an intra-axial lesion in the left parasagittal frontoparietal region measuring 5.3 × 4.3 × 3.0 cm. The lesion was T1 hypointense, T2/FLAIR hyperintense, showed heterogeneous diffusion restriction, and demonstrated heterogeneous post-contrast enhancement. The patient underwent left parietal craniotomy and subtotal excision of the lesion. Histopathology was suggestive of diffuse large B-cell lymphoma, non-germinal center type, with co-expression of BCL2 and c-MYC. She subsequently received chemotherapy.
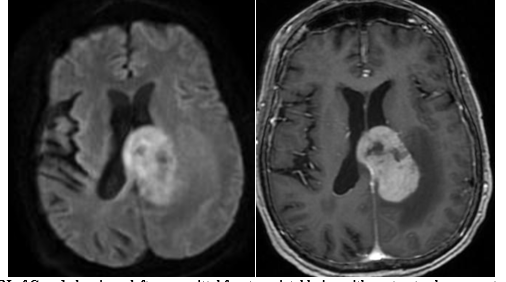
Figure 1: MRI of Case 1 showing a left parasagittal frontoparietal lesion with contrast enhancement and diffusion restriction.
CASE 2
A 68-year-old man presented with holocranial headache, forgetfulness, and slowing of daily activities for one month. On examination, Glasgow Coma Scale score was E4V4M6. Cranial nerve examination was normal, and no motor deficits were noted.
Magnetic resonance imaging showed an ill-defined contrast-enhancing lesion with diffusion restriction in the right gangliocapsular and right parietotemporal region, measuring 1.2 × 1.5 × 1.4 cm. Frame-based stereotactic biopsy was performed. Histopathological examination confirmed diffuse large B-cell lymphoma. The patient was referred for definitive oncological treatment.
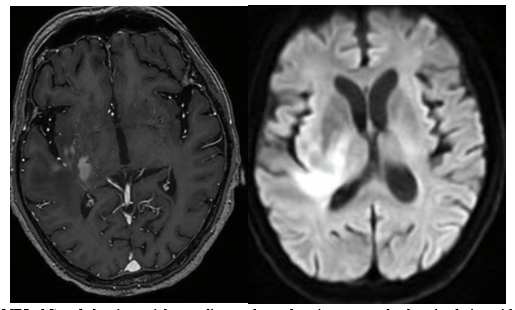
Figure 2: MRI of Case 2 showing a right gangliocapsular and parietotemporal enhancing lesion with diffusion restriction
CASE 3
A 53-year-old woman presented with headache for one month and vomiting for 20 days. On examination, Glasgow Coma Scale score was E4V5M6, pupils were equal and reactive, and no focal neurological deficits were identified.
Magnetic resonance imaging demonstrated multicentric ill-defined T2 intermediate signal intensity lesions involving the body and splenium of the corpus callosum with subtle diffusion restriction and homogeneous post-contrast enhancement. The patient underwent neuronavigation-guided biopsy from the anterior body of the corpus callosum through the left Kocher’s point. Histopathology revealed diffuse large B-cell lymphoma, germinal center type. She subsequently received treatment.
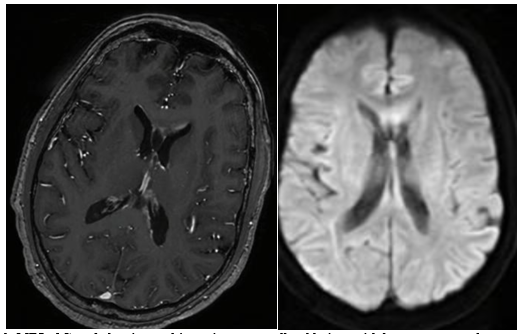
Figure 3: MRI of Case 3 showing multicentric corpus callosal lesions with homogeneous enhancement and diffusion restriction
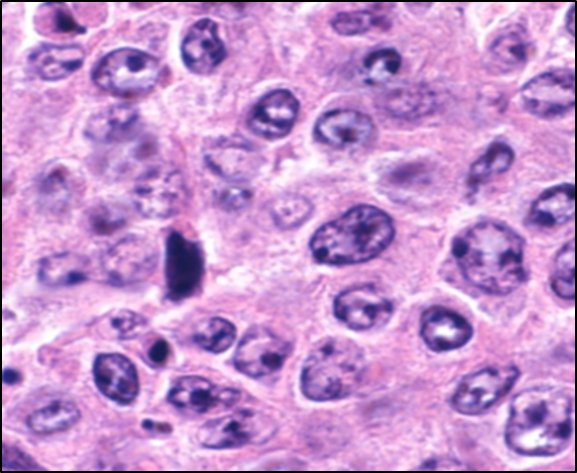
Figure 4: Histopathological image showing neuroparenchyma infiltrated by atypical lymphoid cells with angiocentric distribution
FINDINGS
The age of patients in this series ranged from 53 to 72 years. Headache was present in all three patients, making it the most common presenting symptom. One patient had focal motor deficit, one had cognitive-behavioral slowing, and one had symptoms of raised intracranial pressure without focal deficit.
Magnetic resonance imaging showed contrast enhancement and diffusion restriction in all cases. Histopathology confirmed diffuse large B-cell lymphoma in every patient. Two patients underwent biopsy as the primary diagnostic procedure, while one underwent subtotal resection.
DISCUSSION:
Primary central nervous system lymphoma remains a rare but important differential diagnosis in patients with enhancing intracranial lesions. The lesions often arise in deep-seated structures and may present with non-specific symptoms, which can delay diagnosis.[3,5]
In the present series, headache was the predominant symptom, and all lesions showed contrast enhancement with diffusion restriction on MRI. Restricted diffusion is a useful radiological clue because of the high cellularity of PCNSL, although tissue diagnosis is still required because imaging findings are not pathognomonic.[3]
All three cases in this series were diffuse large B-cell lymphoma, which is in line with published literature identifying DLBCL as the most frequent histopathological subtype of PCNSL.[4,6] The age range in this series also aligns with the known predominance of PCNSL in older adults, although younger immunocompetent patients may also be affected.[2,6]
Current evidence and guideline-based recommendations support stereotactic or neuronavigation-guided biopsy as the preferred neurosurgical strategy in most patients with suspected PCNSL. Unlike high-grade gliomas, extensive resection has a limited routine role because definitive treatment primarily depends on systemic therapy, especially high-dose methotrexate-based regimens.[4,5]
Recent reviews and guidelines continue to support high-dose methotrexate as the backbone of induction therapy, often in multidrug protocols, with consolidation tailored to patient age, performance status, and institutional practice.[4,6] These principles underscore the importance of obtaining a prompt and accurate tissue diagnosis while minimizing unnecessary surgical morbidity.[5]
This series is limited by the small sample size, retrospective design, and absence of long-term outcome analysis. However, it highlights a consistent clinicoradiological pattern and reinforces the value of minimally invasive biopsy techniques for establishing diagnosis in suspected PCNSL cases.
CONCLUSION:
Primary central nervous system lymphoma should be strongly considered in patients with intracranial enhancing lesions that demonstrate diffusion restriction on magnetic resonance imaging. In this series, headache was the most frequent presenting symptom and diffuse large B-cell lymphoma was the histopathological diagnosis in all three patients.
Early histopathological confirmation through stereotactic or navigation-guided biopsy is critical for timely initiation of appropriate oncological therapy. Neurosurgical management should focus on safe tissue diagnosis, after which methotrexate-based chemotherapy forms the cornerstone of treatment in most patients.[4,5]
Funding: Nil.
Conflicts of interest: None.
REFERENCES:
1. Batchelor TT. Primary central nervous system lymphoma. Hematology Am SocHematolEduc Program. 2016;2016(1):379-385. doi:10.1182/asheducation-2016.1.379.
2. Grommes C, DeAngelis LM. Primary CNS lymphoma. J ClinOncol. 2017;35(21):2410-2418.
3. Morell AA, Shah AH, Cavallo C, Eichberg DG, Sarkiss CA, Benveniste R, et al. Diagnosis of primary central nervous system lymphoma: a systematic review of the utility of CSF screening and the role of early brain biopsy. Neuro Oncol Pract. 2019;6(6):415-423. doi:10.1093/nop/npz015.
4. Ferreri AJM, Illerhaus G, Doorduijn JK, Auer DP, Bromberg JEC, Calimeri T, et al. Primary central nervous system lymphomas: EHA–ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024;35(6):491-507. doi:10.1016/j.annonc.2023.11.010.
5. Ferreri AJM, Illerhaus G, Doorduijn JK, Auer DP, Bromberg JEC, Calimeri T, et al. Primary central nervous system lymphomas: EHA–ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. HemaSphere. 2024;8(6):e89. doi:10.1002/hem3.89.
6. Ferreri AJM, Calimeri T, Ponzoni M. Treatment of primary central nervous system lymphoma: current approaches and future directions. Cancer Treat Rev. 2024;128:102781. doi:10.1016/j.ctrv.2024.102781.